

Does the manchester triage system detect the critically ill
|
91 |
|---|
Reducing waiting time at an emergency department using design for Six Sigma and discrete event
simulationAbdallah A. Abdallah
Industrial Engineering Department,
German Jordanian University,
Amman, 11180, Jordan
E-mail: abdallah.abdallah@gju.edu.jo92 N. Mandahawi et al.
Keywords: design for Six Sigma; DFSS; emergency department; ED; triage; length of stay; LOS; waiting time; WT; discrete event simulation; DES; Sigma level; healthcare.
Yousuf Alfarah is a graduate student at the Jordan University, in Amman. His major is in simulation, Six Sigma and design for Six Sigma.
nurse and/or a clerk receives all other patients at the registration desk, registering their names, identification (ID) numbers (similar to social security numbers in the USA) and their arrival times.
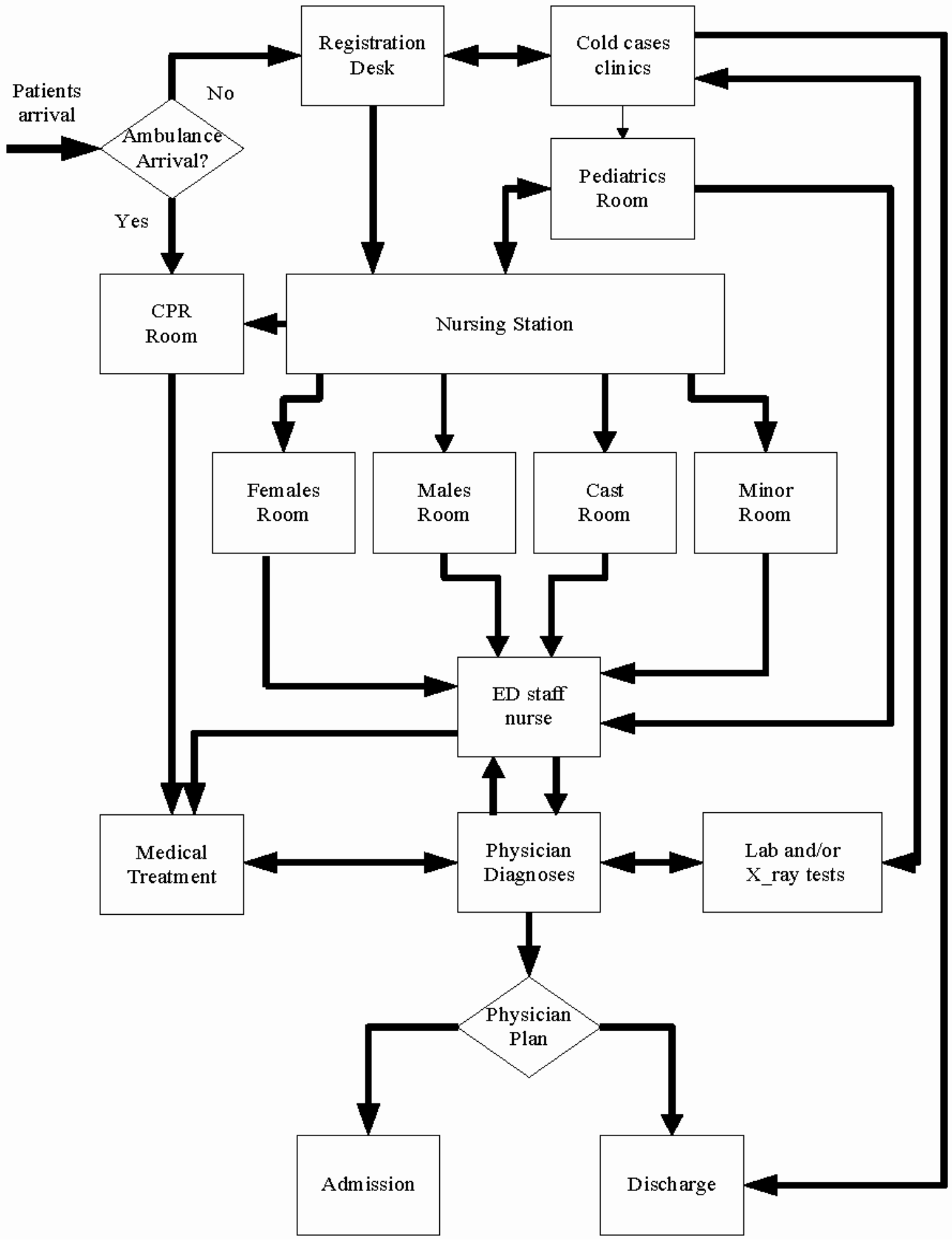
Figure 1 Current flow of patients
 |
|---|
Currently, patients that are issued the same form are most often received and treated based on the policy of first-in-first-out (FIFO), without anyone knowing their illness or pain level. This policy exposes patients to additional health problems due to the waiting time and lack of assessment of their status.
The current procedure has two main disadvantages. Forms are issued based on series of questions asked to the patients and without considering the patient’s vital signs. As a result, there is a significant possibility that the nurse will issue the wrong form, since this procedure depends on a set of direct questions asked to arriving patients. There is only one orientation nurse responsible for issuing forms to all patients. During this study, it was obvious that the nurse issues these forms without knowing the exact complaint for the patient. Because only two forms are used and patients with the same form are treated based on FIFO, patients are routinely exposed to additional health risks due to the significant waiting time before assessment and treatment.
The objective of this paper is to create a triage process that will contribute to reducing patients’ WT and LOS in the ED, using the DFSS with a DES model as an analysis tool.
Reducing waiting time at an emergency department 95
This paper focused on the ED of a specialised hospital and revealed an increase of 75% in patient flow over the last four years. DFSS methodology has been used to define the problem and measure the current sigma level. MTS has been employed to improve the current patient flow by introducing a triage process. Different industrial tools have been used to evaluate current and future scenarios, such as time studies, work flow analyses, VOC, and discrete event simulations. The overall objective is to treat patients based on their illness levels rather than their arrival times, improving process performance by using current available resources.
3 Design for Six Sigma
The process sigma level expected for a DFSS product or service is at least 4.5, but it can be 6 σ or higher, depending on the entity designed (El-Haik and Al-Aomar, 2006). Sigma level is used as a performance indicator in the healthcare service to indicate DPMO that are outcomes from a healthcare process. DFSS involves determining the needs of the customers of a product or service, and driving those needs into the product or service being created.
The voice of the customer (VOC) is a key factor in DFSS because the design of a new product or service process should consider customers’ wants and needs, which is the ultimate objective of the design or redesign process.
In the define phase, the project outlines, metrics, and objectives must be clearly identified. The project charter is a helpful tool in this context. It describes the project scope, goals, and anticipated benefits. Table 1 shows the project charter used to guide this research.
In this paper, WT is defined as the time patients spend in the ED before being seen by a physician, beginning with their registration time. LOS is defined as the total time that patients spend between their registration time and their discharge or admission time.
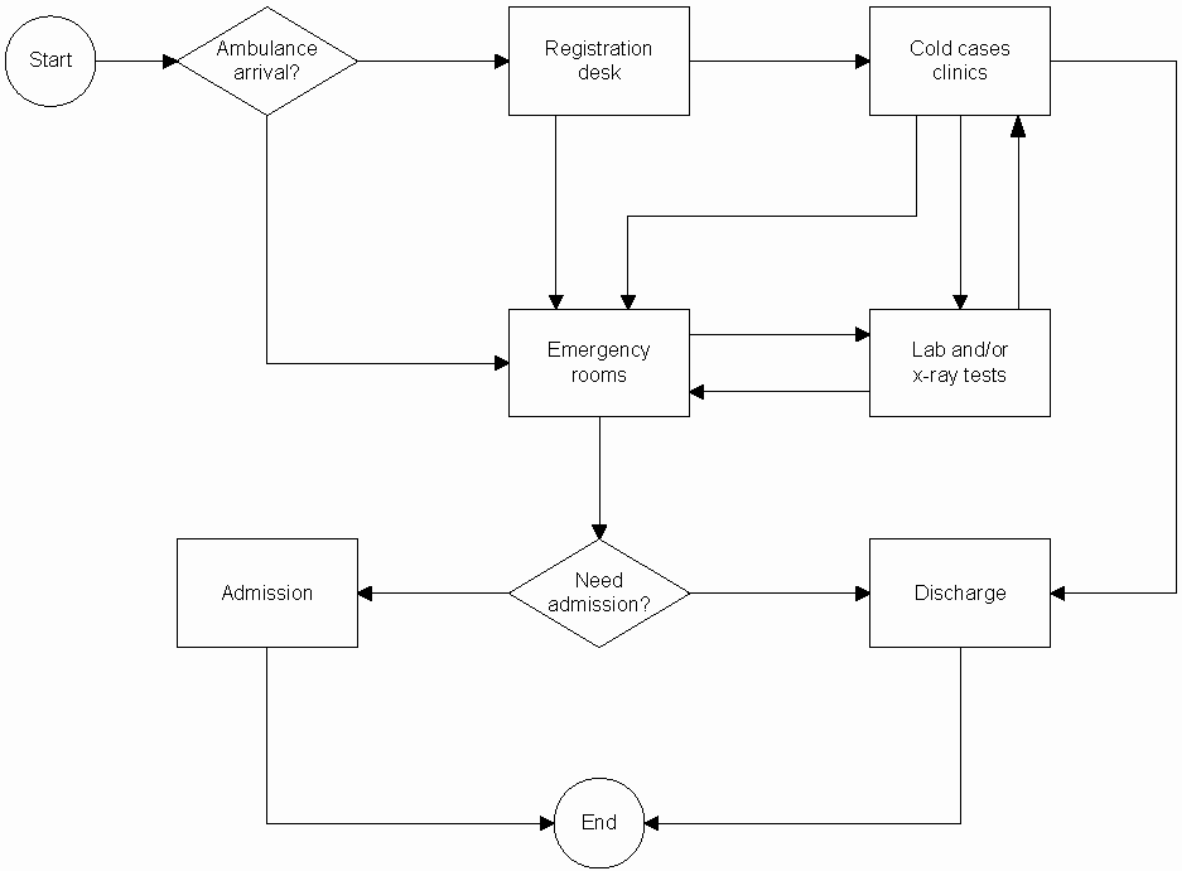
map which indicates that, if patients arrived by ambulance, they will be directed to the emergency rooms. Other arrivals must go to the registration desk to document their personal information.
Depending on their chief complaints, patients will be directed to either the emergency rooms or the cold case clinics. If the physician at the cold case clinics diagnoses a patient as a non-cold case, that patient will be referred to the emergency rooms. In this project, the process terminates once the patient is either discharged or admitted to the hospital.
Description: The triage process is one in which the patient’s illness level is identified. In this project, both DFSS and DES will be used as tools to show the effect of a triage system on reducing LOS and WT.
Background: Data on current ED processes will be collected and analysed to measure WT, LOS, and Sigma level. A simulation model will then be developed to implement and verify the triage process and estimate the new WT and LOS. A new Sigma level will be calculated.
2 Reduce patient’s WT and LOS, which will improve the patient satisfaction
3 Improve the process Sigma level
3.2 The measure phase
The analysis phase deals with identifying the critical factors embedded in the current ED that can be changed to minimise WT and LOS. After data on customer requirements and specifications were collected in the measure phase, CTQ factors and specifications regarding the customer’s VOC became the basis for the design of the triage process.
An analysis of the survey reveals that 81% of the respondents consider the current WT quite long. Furthermore, patient interviews and discussions have been helpful in transforming the VOC into CTQ factors. Data analysis for the patient survey reveals the most important CTQ factors for patients are WT, LOS, lab time, and X-ray time. Patients’ CTQ factors are formulated based on their VOC. Table 2 reveals that the most important VOC for patients is to reduce WT to less than 20 minutes and LOS to less than
| Table 2 | Patient CTQ factors and the specifications of the VOC | ||
|---|---|---|---|
| CTQ | |||
|
WT |
|
|
| LOS | |||
The primary Y’s for this study are WT and LOS. Y’s are affected by many variables: X’s, such as the presence of triage process, the number of physicians, the number of nurses, physicians’ experience levels, nurses’ experience levels, diagnosis time, treatment time, and the current layout. In order to identify which X variables have the highest impact on CTQ factors, quality function deployment (QFD) will be used to identify these factors.
| Table 3 | Patients’ QFD | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| H = 9 | Importance | Registration | Triage | Nurse | assessment | Physician | diagnosis | Medical | treatment | Lab | department | X-ray | department | Pharmacy | Total |
| M = 3 | |||||||||||||||
time
| Reduce X-ray | 3 | 4 | M | 49 | L | L | 39 | H | 4 | 42 |
|---|---|---|---|---|---|---|---|---|---|---|
|
||||||||||
| 99 | 55 | 15 | 39 | 304 |
Based on the QFD tool, the triage process will be the core process in the ED. The triage station will be located where a triage nurse can monitor both the arriving patients who must be triaged and patients who have been triaged and are waiting for medical treatment. A new patient flow will be developed using the triage concept, as shown in Figure 3.
patient’s situation to identify illness level. Based on this assessment, patients will be issued a coloured tag attached to their medical file that will reflect their sickness level. Table 4 shows the triage tag colours and the estimated WT associated with each colour. These recommendations are based on the international MTS system.
At the triage station, the triage nurse will identify patients’ vital signs, take a brief history of their complaints, take electrocardiogram (ECG) readings, order lab tests and/or X-rays, and give injections or medications to relieve pain. All of these actions will be taken under the signature of an ED physician.
While they are waiting, patients who require lab tests or X-rays can get these procedures done. When they get the results, they can return to the waiting desks and continue to wait for the necessary care. This procedure is helpful in reducing WT and LOS, since WT for a physician currently includes waiting for lab tests and X-rays. Except for special tests ordered by the EP, all patients will be ready for diagnosis and treatment by a physician based on vital signs and the assessment carried out by the triage nurse.
3.4.2 Developing the DES model
| Table 5 |
|
||
|---|---|---|---|
|
Tag name | Expected number | |
| Emergent | |||
| Very urgent | |||
| Urgent | |||
| Green | Normal | ||
|
Cold | ||
Harrel et al. (2004) stated that simulation models can be verified through conducting a model code review, watching the animations for correct behaviour, and using the trace and debugging features provided with the software. Consequently, in this paper, a simulation model has been developed, warmed up, and verified by tracing patients, physicians, and nurses. The model’s outcomes are within reasonable limits. It never outputs abnormal results, and a review of the model code ensures that the model has been correctly verified.
3.5 The verify phase
The verify phase consists of implementing the triage process. The validated triage DES model has been used to verify the triage process. The reported results represent the average of 96 runs. An appropriate warm-up period has been eliminated from these runs.
| Table 7 | |||
|---|---|---|---|
| Variable | Current state Sigma level | Triage state Sigma level | |
| 0.66 | |||
|
0.58 | ||
| 4 |
|
||
Choi, F., Wong, W. and Lau, C. (2006) ‘Triage rapid initial assessment by doctor (TRIAD) improves waiting time and processing time of the emergency department’, Emergency Medicine Journal, Vol. 23, pp.262–265.
Cooke, M.W. and Jinks, S. (1999) ‘Does the Manchester triage system detect the critically ill?’, Journal of Accident & Emergency Medicine, Vol. 16, pp.179–181.
Harrel, C., Ghosh, K. and Bowden, O. (Eds.) (2004) Simulation using ProModel, McGraw-Hill, New York.
Jones, K., Marsden, J. and Windle, J. (Eds.) (2006) Emergency Ttriage: Manchester Triage Group, BMJ Publishing Group, Oxford.
Stritto, R.A. (2005) ‘The experience of the emergency triage nurse: a phenomenological study’, PhD dissertation, Texas Women’s University, Denton, Texas, USA.
Winn, K. (2001) ‘Emergency department efficiency through utilization of triage nurse protocols’, Master thesis, Texas Tech University Health Science Center, Texas, USA.




