Australian government programs targeting development of the rural workforce
OUR VISION |
|---|
2.1 MOUs – operational phases and jurisdiction coverage 4
2.6.1 Initiative participation 6
2.10.1 Health workforce supply 17
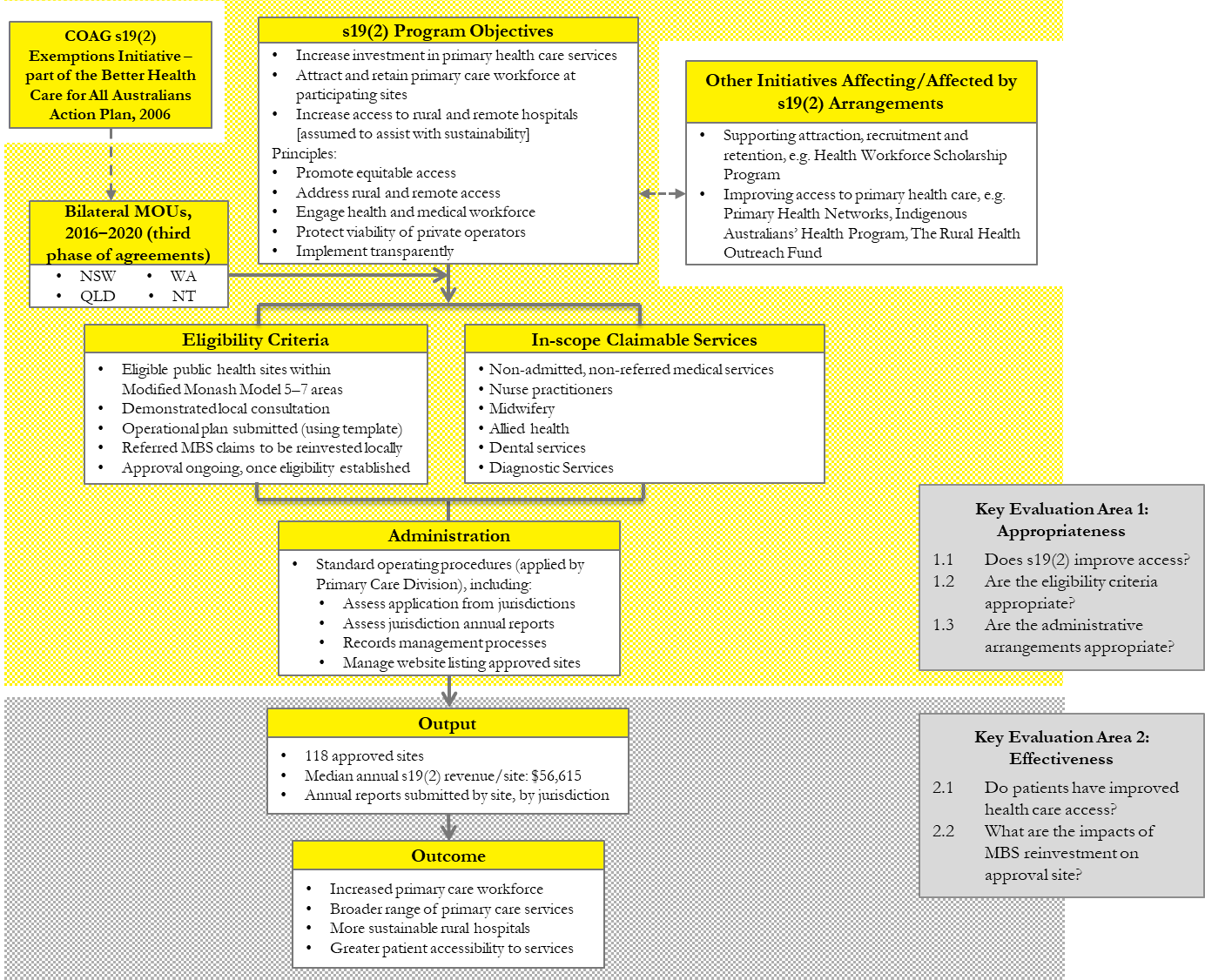
3.1 Specifying the program logic and evaluation areas 21
Part B Evaluation Findings & way forward 27
4.3.1 Relative contribution of Initiative revenues to service budgets 37
4.3.2 Importance of the Initiative to sustainability: normative assessment 40
4.5.1 Principles: Value and contribution 42
4.5.2 Site engagement of stakeholders 43
4.7 MBS billing – site & LHN processes 48
Option 1: Administrative refinement of the Initiative 58
Appendix A Detailed evaluation questions specified in the RFQ 64
Appendix B List of other S19(2) Exemption sites 65
Abbreviations
supporting participating sites to attract and retain a relevant primary healthcare workforce, and
assisting with the sustainability of rural hospitals.
Medical Benefits Schedule (MBS) rebates received by sites under the Initiative in 2019–20 totalled $13.6 m.
Evaluation requirement and approach
‘undertake a robust review of the COAG Section 19(2) Exemptions Initiative – Improving Access to Primary Care in Rural and Remote Areas (the Initiative) – to determine how the Initiative achieves its objectives’
Evaluation objectives and method
Stage 3: Evaluation plan: the plan finalised the evaluation questions, specified data sources and data collection protocols, and designed collection tools.
Stage 4: Data collection: HMA collected a range of qualitative and quantitative data via surveys and interviews conducted with relevant stakeholders. We sought insights into the effectiveness of the Initiative from a range of stakeholder perspectives.
Context: Overview of the Initiative
The MOUs specify the rules for operation of the Initiative, including:
Approval to participate, services that are eligible to be claimed, and rules for the reinvestment of MBS rebated revenue
Reporting arrangements for participating sites.
The wider context for the Initiative influences what happens ‘on the ground’ at individual participating sites, including:
Broader developments in the health and human delivery in the areas of the National Disability Insurance Scheme, the Royal Commission into Aged Care, and pilots funded under the new National Health Reform Agreement 2020–2025.
Patterns of service delivery under the Initiative
Although the program website lists 118 participating sites, only 92 of those sites were paid MBS revenue in 2019–20.
these eight sites accounted for revenue of $6.3 million under the Initiative, more than 45% of total funds generated, and
three of these sites were in WA, four in Queensland and one in NT.
Evaluation findings
Program design and administration
Appropriateness
Consideration of the Initiative’s appropriateness observed that funding contributions to different sites resulting from the Initiative can be internally inequitable – larger sites with more salaried doctors have a greater ability to undertake MBS billing.
This characteristic highlights a program impact that emerges from its inherent design; MBS revenues of a site are not directly linked to underlying health needs of a community.
Effectiveness
The way forward: Options for program refinement
The findings from the evaluation suggest that changes to the current arrangements should be considered to ensure implementation of the Initiative:
is responsive to the context in which it is operating,
Revised program governance arrangements (Option 2) that expand formalised and required engagement via:
Option 2 (a): sub-regional (site level) governance committees, including stakeholders not currently specified in the MOU, such as RWA representatives and local community members, and
During stakeholder discussions for the evaluation there was some support for larger changes to funding arrangements for small health services in rural and remote areas. These options for funding redesign included:
Pooling of funds at a sub-regional level using revenues from the Initiative together with other relevant programs including RWAs, PHNs, NDIS, aged care, local government and LHNs, and
Next steps
Background
Initiative context
Section 19(2) of the Health Insurance Act, 1973 precludes state and territory health services claiming Medical Benefits for non-admitted, non-privately referred services delivered in hospitals, multipurpose services and community clinics. However, in 2006–2007 the Council of Australian Governments (COAG) introduced the Section 19(2) Exemptions Initiative – Improving Access to Primary Care in Rural and Remote Areas (the Initiative) with the objectives of:
In December 2020 there were 118 sites across four jurisdictions (New South Wales, Queensland, Western Australia and the Northern Territory) listed as participating in the Initiative [1]. Medical Benefits Schedule (MBS) rebates received by jurisdictions under the Initiative in 2019–20 totalled $13.716 m.1
The Australian Government Department of Health (the Department) engaged Healthcare Management Advisors (HMA) to
‘undertake a robust review of the COAG Section 19(2) Exemptions Initiative – Improving Access to Primary Care in Rural and Remote Areas (the Initiative) – to determine how the Initiative achieves its objectives’
Are current COAG Section 19(2) Initiative eligibility criteria appropriate to achieve the Initiative’s objectives?
Are current administrative arrangements and processes appropriate for management, accountability and transparency purposes?
Part A: Context
Chapter 1 (this chapter): background on the evaluation
Chapter 5: the way forward– options for program development based on the evaluation findings. The final report includes a summary of jurisdiction’s observations on each option.
Additional background on the scope of the Initiative and relevant data that supported the evaluation analysis is given in the Appendices ( see Chapter 6).
Overview of the Initiative
The broader health and human services context that affects local planning for primary health service delivery, including:
further Commonwealth programs that improve access to primary healthcare, including Primary Health Networks, Indigenous Australians’ Health Program, and the Rural Health Outreach Fund, and
MOUs – operational phases and jurisdiction coverage
The number of participating sites has gradually increased and currently there are 118 approved eligible sites across four jurisdictions – New South Wales, Queensland, Western Australia, and the Northern Territory. Two further jurisdictions are not fully engaged:
South Australia continues to have an MOU with the Commonwealth but has yet to submit any site applications, and
Initiative objectives
‘it recognises that there are challenges in attracting and retaining adequate primary health care providers in rural and remote areas …’
The Initiative therefore:
Principles
Australians in rural and remote communities face particular challenges when it comes to accessing appropriate health care, and it is the responsibility of all Australian governments to seek to address these challenges.
The health and medical workforce is a finite and valuable resource and its members’ involvement and support is crucial to the continued success of the Initiative.
Program rules
The MOUs specify the rules for target locations, consultations required to obtain approval to participate, services that are eligible to be claimed, and rules for the reinvestment of MBS rebated revenue. The rules state the following:
Consultation with other providers: representatives of the proposed site obtain support for the Initiative operating in a locality from other local primary health care providers (including general practitioners), the Royal Flying Doctor Service (RFDS) and Aboriginal Health Services (AHS).
Standard Operating Procedures
The Primary Health Care Governance and Implementation Section, Primary Care Division, has a suite of Standard Operating Procedures (SOPs) to inform Department processes for managing the program. This document re-states much of the MOU contents but has additional processes and guidance on:
assessing applications lodged by jurisdictions and protocols for communication of decisions back to jurisdictions and updating the website list of approved sites
The Assistant Secretary of the MBS Policy and Specialist Services Branch, Medical Benefits Division has delegation under this Instrument to approve exemptions under the Initiative. Exemptions are granted through Directions for the Initiative.’ [3]
Patterns of delivery
Initiative participation
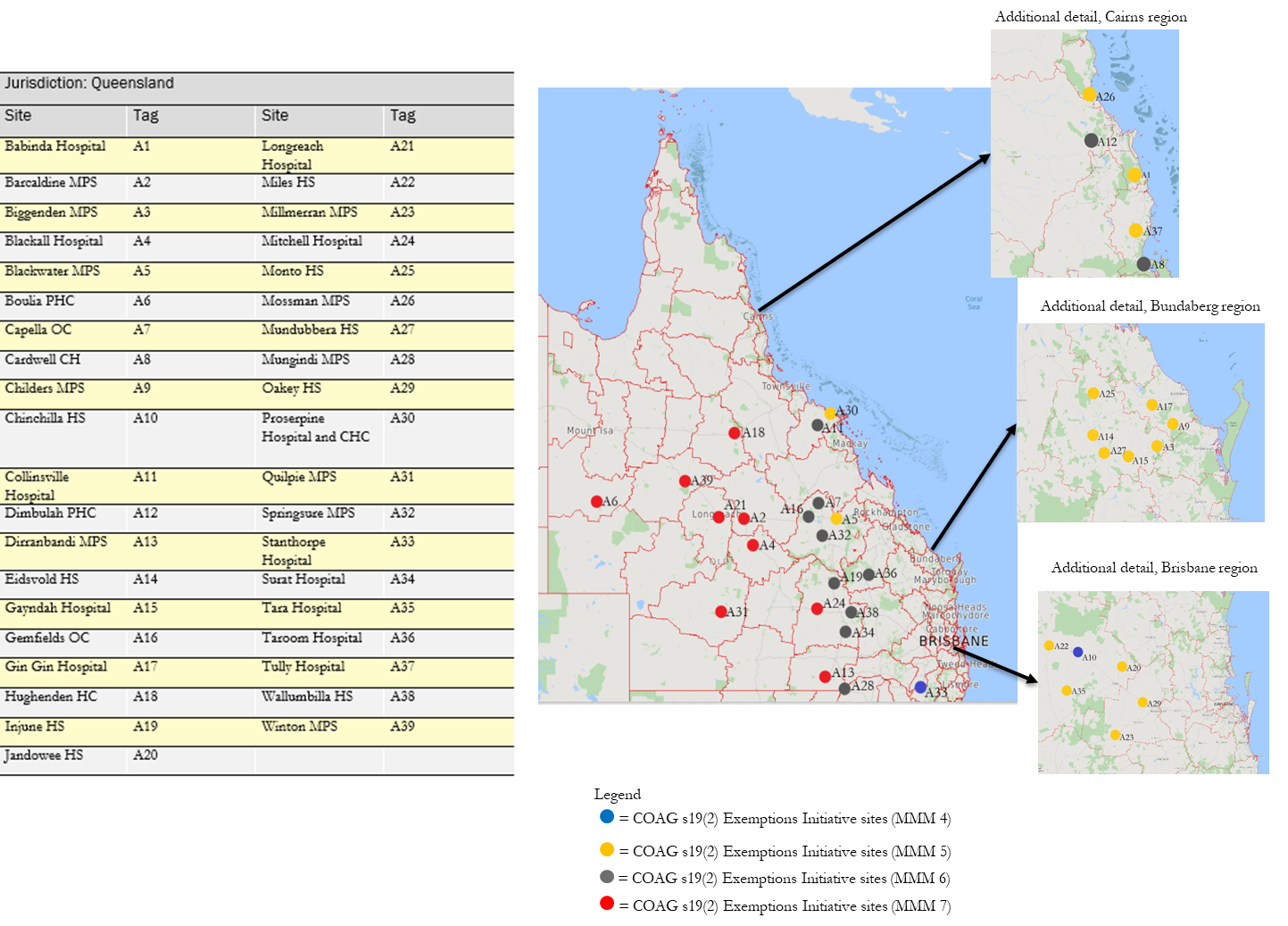
Although the program website lists 118 participating sites, only 92 of those sites were paid MBS revenue in 2019–20. Table 2.1 shows the number of those active sites by jurisdiction and categorises their MMM ratings.
| MMM score | NSW | Qld | WA | NT | total | MMM Score % |
|---|---|---|---|---|---|---|
| 4 | 2 | 2 | 2 | |||
| 5 | 33 | 17 | 50 | 54 | ||
| 6 | 3 | 11 | 3 | 17 | 18 | |
| 7 | 9 | 11 | 3 | 23 | 25 | |
| Total | 36 | 39 | 11 | 6 | 92 | 100 |
| 39 | 42 | 12 | 7 | 100 |
Source: Unpublished Department data – MBS payments data
The table shows that: New South Wales and Queensland had the most participating sites, having 36 and 39 active sites respectively in 2019‒20, representing 81% of the 92 active sites. Western Australia had 11 active sites (12% of the total) and Northern Territory had 6 active sites (7% of the total).
Figure .: Location of Queensland Initiative sites receiving MBS revenue, 2019‒20
MBS claims
In 2019‒20 the 92 active sites received MBS rebates totalling $13.6 m. They had a median rebate of $56,081 (see Table 2.2).
Table .: Median size of MBS rebate by jurisdiction, 2019‒20
Impact of doctor remuneration arrangements on MBS billing
Queensland: in rural and remote Queensland, Local Health Networks (LHNs) known as Hospital and Health Services (HHSs) employ doctors to staff local hospitals to provide acute, inpatient, outpatient and emergency care. Doctors in small rural hospitals are now predominantly employed as Senior Medical Officers (SMO) (largely replacing the Medical Superintendent and Medical Officer Right to Private Practice arrangement). A right of private practice assignment model generally operates in non-metropolitan hospitals, whereby an allowance is paid to the SMO and all private practice revenue is paid to HHS. [4] Under the Medical Officers’ (Queensland Health) Certified Agreement (No. 5) 2018 [5] SMOs receive a loading applied to the base salary where they are billing MBS revenue, historically set at 25% of salary.
New South Wales: private GPs provide community based and hospital care remunerated under a Medicare fee-for-service model for office-based care. Remuneration is under the terms of the New South Wales Rural Doctors Association (RDA) Settlement Package. [6] This establishes payment rates for medical services provided by GP Visiting Medical Officers (VMOs) at 125 small hospitals in rural NSW, specified in the Package. These payment rates are only available to RDA (NSW) members and are substantially higher than the Medicare rebates otherwise payable. The package ensures that GP VMOs providing on-call and after-hours services in areas with minimal specialist backup are renumerated appropriately for the services they provide. The VMO services to the local hospital may include procedural and inpatient services, emergency care triage categories 1–3, and on-call services (dependent on their credentialing and scope of practice).
In the northern half of the state, the predominant remuneration and employment model is salaried medical officers employed by the Western Australian Country Health Service (WACHS). Under the terms of the WA Award, salaried medical officers at WACHS facilities can elect to retain up to 25% of the practitioner’s salary from nett earnings from private practice within the hospital.2 Private general practice is very limited across the remote communities of northern Western Australia. ACCHOs operate in many communities in the Kimberley, the Pilbara, and Geraldton.
Nursing and allied health workforce
Other Section 19(2) exemptions in rural communities
The Aboriginal Community Controlled Health Services Section 19(2) Direction managed by the Indigenous Health Division
The Remote Vocational Training Scheme Direction, managed by Health Workforce Training.
It is important to understand the breadth of Section 19(2) exemptions in place, their specificity, the rural and remote communities in which they operate and the potential intersection with the COAG Section 19(2) Initiative. We provide an overview below. The services where these arrangements apply are listed, by jurisdiction, in Appendix B.
The Aboriginal Community Controlled Health Services Direction
ACCHOs operate on a resident or visiting basis in some of the listed COAG Section 19(2) exempt sites in New South Wales, Western Australia, Queensland and Northern Territory. At these sites, the ACCHO may provide medical, allied health and/or nursing services. Some also offer dental services, which may be under an arrangement with an LHN, university dental school, or philanthropic organisation. ACCHOs are increasingly reliant on Medicare income to support and expand their service offerings.
The Queensland State Government (Indigenous Health) Direction
This Direction allows Medicare benefits to be payable in respect of:
The Northern Territory
Non-referred professional services provided by salaried medical practitioners, participating midwives and participating nurse practitioners, and
Referred professional services provided by salaried allied health and dental health professionals, optometrists, Aboriginal and Torres Strait Islander Health Practitioners and Aboriginal health workers.
Murrumbidgee Local Health District Direction
the service is provided by a participating rural generalist trainee who is centrally employed by the Murrumbidgee LHD for the provision of primary and acute care and is registered in the rural generalist’s innovative employment model trial within the Murrumbidgee region.
This Direction was issued on 19 October 2020 and has effect until 31 December 2024.
Remote Vocational Training Scheme Direction
While the Direction indicates that sites will be in a rural and remote practice location in MMM 4‒7, the currently approved sites are in MMM 5, 6 and 7 and in Tasmania (Smithton), Victoria (Robinvale), New South Wales (Cobar, Lake Cargelligo), Queensland (Clermont, Mt Isa, Badu Island), South Australia (Streaky Bay, Cleve, Kimba, Elliston, Cowell) and Western Australia (Fitzroy Crossing).
The Direction commenced 21 January 2021 and has effect until 31 December 2021.
Rural policy context
Health workforce supply
The Australian Government has introduced a range of policies to address health workforce shortages. Supply strategies have included recruitment of internationally trained medical graduates (IMGs) and other health professionals; doubling the number of medical school places in 2006; and, in response to the Review of Higher Education (Bradley Review) [9], uncapping university training places for nursing and allied health students.
Nationally, there were 410.4 FTE doctors per 100,000 residents in 2017 compared with 382.1 FTE per 100,000 in 2013. In 2017, the nursing and midwifery workforce totalled 284,120 FTE or 1,154.9 FTE per 100,000 residents, which was similar to the 2013 levels on a per population basis. However, the supply of allied health practitioners registered with the Australian Health Practitioner Regulation Agency (AHPRA) increased in the period 2013 to 2017 from 98,545 FTE (426.1 FTE per 100,000 residents) to 114,606 FTE (465.8 FTE per 100,000. [10])
While the specialist-GP FTE rate (per 100,000 population) is relatively higher in remote and very remote areas, this figure does not reflect population dispersion nor residents’ ability to access services. The Geographic Index of Relative Supply (GIRS) adjusts the known workforce supply for land size, population dispersion and proximity of the population to relevant service locations. GIRS scores range from 0 to 8. Areas with lower GIRS scores are more likely to face workforce supply challenges than those with higher scores. Figure 2.7 illustrates that relative to major cities, remote and very remote areas of Australia face substantially higher GP workforce supply challenges.
Figure .: GIRS index scores, Specialist General Practitioners by Statistical Area (SA2) (2014)
Initiatives supporting attraction, recruitment and retention
Improving access to primary healthcare
In addition to Medicare, the Australian Government predominantly invests in the support of primary healthcare through Primary Health Networks (PHNs) and ACCHOs.
Primary Health Networks (PHNs)
The Rural Health Outreach Fund (RHOF) aims to improve access to medical specialists, GPs, allied and other health providers in rural, regional and remote areas of Australia. The RHOF, introduced in 2011, consolidated the activities of five existing outreach programs:
Medical Specialist Outreach Assistance Program (MSOAP)
There are four health priorities under the RHOF: maternity and paediatric health, eye health, mental health and support for chronic disease management. Rural Workforce Agencies (RWAs) manage the RHOF in each jurisdiction other than Queensland – where it is managed by Check-Up.
Intersection with the Section 19(2) Initiative
Wider health and human services context
The new National Health Reform Agreement 2020–2025 was signed off by all Australian governments in May 2020. Through this agreement, the Australian Government contributes funds to the states and territories for public hospital services. This includes services delivered through emergency departments, hospitals and community health settings.
The long-term reforms outlined in the 2020–2025 agreement will examine how well the different components of the health system interact. The reforms will give local health services the flexibility to try new solutions to address system barriers and improve service delivery to ensure health services best suit the needs of their local community. The six reforms focus on:
Enhanced health data – integrating data to support better health outcomes and save lives, and
Nationally cohesive health technology assessment – improving health technology decisions will deliver safe, effective and affordable care.
Evaluation approach
The conduct of case studies, and
A survey of Initiative participating sites.
Specifying the program logic and evaluation areas
Process (the how)
Outputs, which can be quantifiable measures
Evaluation method
The review comprised the following eight project stages:
determined data sources and data collection protocols
designed data collection tools
internal Department of Health stakeholders
all jurisdictions (both participating and non-participating)
submissions on the operation of the Initiative from
the Rural Doctors Association of Australia (RDAA) and its affiliates, and
annual reports from participating sites
standard operating procedures
other relevant data gathered throughout the evaluation.
Stage 7 – Information synthesis: (June 2021) The project team triangulated findings from the previous stages and formed evaluative judgements of Initiative performance against the evaluation questions specified in Attachment A. This enabled an assessment of the extent to which the Initiative is appropriate, effective, efficient and of quality and value.
Specific data collection processes: additional information
MBS data analysis
Midwifery
Allied health
Social Work
Other
Case studies
senior management representatives of the LHN responsible for the participating case study health service
the facility manager
local GPs and representative of ACCHOs, where present and available.
The evaluation analysis drew on more detailed information on each case study site made available from the Department:
Table 3.1: COAG S19(2) Exemptions Initiative evaluation case study sites – summary of contextual features
| Jurisdiction | Case study site name / MBS Claim ‒ $m (2019/20) | Nearest large town | LGA population | MMM score | No. of private GP clinics in town | Most proximate ACCHO | Rationale for inclusion as a case study |
|---|---|---|---|---|---|---|---|
|
|
|
|||||
|
|
||||||
|
|
|
|||||
|
|
||||||
|
Airlie Beach |
|
|
||||
|
|
||||||
|
|
|
|||||
|
|
|
|||||
|
|
||||||
|
|
|
Survey of participating sites
how the MBS revenue was reinvested at the site over the period of the 2016– 20 MOU, and
the full time equivalent (FTE) staffing levels at the site on 30 June 2020 (including management, administration, clinical and non-direct care staff, e.g. cleaners, catering).
Evaluation Findings & way forward
Evaluation findings
In this chapter we provide our evaluation observations and findings. The evaluation analysis addresses the key evaluation questions specified in the project RFQ and incorporates three broad areas of examination: effectiveness, program administration, and appropriateness.
Access to primary care
After-hours non-referred attendances (including items 5000, 5020, 5040 and 5060) – $3.6 m in payments (26.3% of the total) with a median payment of $19,515 per service.
Review of operational plans at case study sites shows the bulk of these consultations were for urgent and/or emergency medical care.
greater use of the after-hours items in NSW (60.1% of jurisdiction claims), but less use of the assessment and other professional items (0.6% of jurisdiction claims)
WA sites made the least use of the after-hours items (13% of jurisdiction claims)
Source: MBS Data Extract, 2019–20, prepared for HMA Evaluation.
Definitions for MBS item numbers included in each aggregated category are given in Appendix E.
Has the Initiative ensured access to urgent and/or emergency medical care? Typically, in a small rural town (MMM 5 or higher), available medical care should include access to a medical practitioner on call or available via telehealth during daytime hours (see for example [15]), and
Has the Initiative ensured access to integrated, comprehensive primary care? Such services should include provision of general practitioner care in association with nursing and allied health practitioners to deliver care management plans, chronic disease management, community-based mental healthcare, maternal and child health, women’s health, family planning, and support for lifestyle management. The overall objective of integrated services should be to promote health and wellbeing, assist people to rehabilitate and recover, and to support people to live at home. [16]
there were limited referral pathways to other locally based primary care clinicians for ongoing management beyond the acute presentation. This lack of referral was not surprising because at several of these case study sites there were limited numbers of nurse practitioners and/or allied health practitioners available to support non-acute needs.
Table 4.2: Evaluation case study sites – local characteristics of access to primary care
| Measure of Access to Primary Care | Queensland | New South Wales | Northern Territory | Western Australia | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Tully | Longreach | Proserpine | Temora | Nyngan | Quirindi | Tennant Ck | Jabiru | Kununurra | Meekatharra | |
| The Initiative claims: 2019‒20 | $0.660 m | $0.258 m | $1.300 m | $0.300 m | $0.050 m | $0.040 m | $0.600 m | $0.200 m | $0.200 m | $0.070 m |
Score 3 The Initiative added to the number of doctors at the health service |
Score 0 Virtual Rural Generalist (VRG) program, with only 1 week in 6 on-site face-to-face; not making major difference to emergency care availability |
Score 3 The Initiative ensured funding of 24 hours ED service |
Score 2 Private practice in town; patients sometimes choose to present to ED rather than private practice |
|||||||
| The Initiative contributed to Integrated comprehensive primary healthcare (e.g. chronic disease management, lifestyle management, mental health, child health) | Score 3 PHOs funded by the Initiative undertook 6-month rotations in private GP practices, in addition to 6 months in ED |
Score 0 Developmental model of care at this stage with intention around care navigation and workforce development |
Score 1 Podiatrist (private provider) and antenatal outreach nurse provide some broader primary care services |
|||||||
Proserpine Hospital: using the Initiative to improve access to emergency care
Proserpine Hospital is a 33-bed facility that has day surgery capacity and a community health centre. The immediate town has a population of 3,500 people but the hospital is the major source of acute care, including emergency care, for a regional population of 34,000 people, including the large coastal tourist town of Airlie Beach (10,000 people) 30 km to the east, and multiple tourist resorts in the nearby Whitsunday Islands. There are two private practices in Proserpine with 6 FTE GPs. These GP services were closed on weekends and did not provide services after hours or on weekends. Prior to the Initiative commencement at the site, after-hours emergency care for the Whitsunday catchment was available from Proserpine Hospital’s 2 FTE Principal House Officers (PHOs). These positions struggled to deal with the volume of after-hours presentations.
65% of managers considered they had adequate access to integrated comprehensive primary care (defined in the survey as GP services plus all other primary health workers and equipment required to address the holistic primary care needs of patients). There was some variation in this response rate by jurisdiction with a low of 43% (n=23) in NSW and a high of 100% in WA (n=11).
Table 4.3: Assessment of adequacy of local service availability at Initiative sites, % ‘Yes’/’No’ for urgent medical care & integrated comprehensive primary care
| Assessment of local service adequacy | Yes | No | n |
|---|---|---|---|
| Adequacy of local urgent medical care (i.e., category 4 and 5 presentations in the ED) | |||
| All responses (NSW, QLD, WA, NT) | 98% | 2% | 47 |
| Adequacy of integrated comprehensive primary care (i.e., GP services plus all other primary health workers and equipment required to address the holistic primary care needs of patients) | |||
| All responses (NSW, QLD, WA, NT) | 65% | 35% | 48 |
| NSW responses | 43% | 57% | 23 |
| QLD responses | 63% | 38% | 8 |
| WA responses | 100% | 0% | 11 |
| NT responses | 83% | 17% | 6 |
Access to primary care: Summary assessment
Based on the analysis presented above, the evaluation team reached the following conclusions:
Analysis of MBS claims, case study site observations and the survey of participating sites found that the Initiative has improved access to urgent/emergency medical care and after-hours services at many participating sites.
Access to relevant healthcare workforce
| Service | Total Initiative funds |
Breakdown of reinvestment of Initiative funds(a) | |||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
|
||||||||||||||||||||
|
|
||||||||||||||||||||
| $ | $ | % | $ | % | $ | % | $ | % | $ | % | $ | % | $ | % | $ | % | $ | % | $ | % | |
| Temora NSW | 141,642 | 45,590 | 32 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 9,065 | 6 | 0 | 0 | 0 | 0 | 76,987 | 54 | 10,000 | 7 |
| Quirindi NSW | 14,272 | 14,272 | 100 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Nyngan NSW | 46,413 | 13,924 | 30 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 10,940 | 24 | 21,549 | 46 |
| Kununurra WA | 271,547 | 97,458 | 36 | 0 | 0 | 0 | 0 | 47,321 | 17 | 33,680 | 12 | 90,904 | 33 | 0 | 0 | 2,185 | 1 | 0 | 0 | 0 | 0 |
| Meekatharra WA(b) | 0 | 0 | n/a | 0 | n/a | 0 | n/a | 0 | n/a | 0 | n/a | 0 | n/a | 0 | n/a | 0 | n/a | 0 | n/a | 0 | n/a |
| Jabiru NT | 204,525 | 10,983 | 5 | 102,263 | 50 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 13,001 | 6 | 0 | 0 | 4,650 | 2 | 73,629 | 36 |
| Tenant Creek NT | 1,205,841 | 0 | 0 | 555,762 | 46 | 173,565 | 14 | 240,132 | 20 | 0 | 0 | 236,382 | 20 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Tully QLD | 639,293 | 133,295 | 21 | 379,499 | 59 | 0 | 0 | 126,500 | 20 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Longreach QLD | 274,674 | 86,403 | 31 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 188,271 | 69 |
| Proserpine QLD | 1,157,700 | 217,671 | 19 | 826,462 | 71 | 0 | 0 | 106,890 | 9 | 0 | 0 | 0 | 0 | 2,727 | 0 | 0 | 0 | 3,950 | 0 | 0 | 0 |
| Total: | 3,955,908 | 619,596 | 16 | 1,863,985 | 47 | 173,565 | 4 | 520,842 | 13 | 33,680 | 1 | 336,351 | 9 | 15,728 | 0 | 2,185 | 0 | 96,527 | 2 | 293,449 | 7 |
(a) Percentages are a proportion of MBS funding (second column)
(b) Meekatharra annual report contained nil data on reinvestment, due to changed model of care arrangements, including attracting a GP to the town to deliver private practice GP services and on-call emergency services of the hospital.
Analysis of the case study experiences indicated that the Initiative investment in allied health and nursing was limited. Investment in allied health occurred at three case study sites and accounted for 10% of total case study revenue reinvested. At similarly low levels was investment in nursing, which accounted for 13% of overall revenue reinvestment, but at only four case study sites. There was negligible investment in professional development and staff training across the case study sites (under 2% of reinvested Initiative funds).
An illustration of how reinvestment of Initiative funds was used to support the development of a healthcare workforce relevant to local needs is provided by Gundagai MPS (see the Case Study Box #2).
To support the sustainability of primary care and secondary care services in the community and build service delivery capacity, the Medical Centre has negotiated an agreement with the Murrumbidgee LHD to guarantee 24/7 coverage to Gundagai MPS by payment of a fixed amount of revenue generated through the Initiative. The practice has used the Initiative revenue to contribute to employment of a Nurse Practitioner (1 FTE) and mental health nurse (0.6 FTE) within the practice supporting the development of an in-house multidisciplinary team, increased capacity for GP care planning and enhanced primary care, improved continuity of care, and further contributing to practice sustainability through Medicare generation.
Investment in equipment to support service delivery predominantly occurred at NSW case study sites but was negligible overall. The case study sites attributed equipment as a suitable way of allocating funds at NSW because of the generally lower average levels of funds at these sites (e.g. $46,413 funds available at Nyngan). Where average funds were lower, there was less incentive to invest in workforce and so greater propensity to invest in equipment.
Table 4.6: Assessment of the Initiative as an effective way to contribute to the attraction and retention of the primary care workforce
Source: evaluation survey of Initiative site managers, question 9
Access to relevant healthcare workforce: Summary assessment
Case study consultations found that the Initiative has been used to support employment of junior doctors in hospitals as a component of Rural Generalist training in Queensland. A separate S19(2) exemption (not formally part of the Initiative) is trialling a single employer model to support RG training in NSW, with a focus on GP exposure and in-reach to hospitals. Consultations with peak body stakeholders, including RWAs, found a strong interest in further exploration of these more flexible employment arrangements.
Development of sustainable health services
The third objective of the Initiative is to assist with the sustainability of rural health services. The evaluation assessed performance against this objective from several perspectives:
Relative contribution of Initiative revenues to service budgets
A comprehensive analysis of the relative size of Initiative revenues to the overall budgets of services would require examination of the profit and loss statements for each site. Such an analysis would require an assessment of financial report comparability across sites (e.g. approaches to treatment of depreciation and salary on-costs), information on processes for the allocation of LHN overheads to individual sites, adjustments to accounts to ensure cross-site comparability, and extensive data collection processes from all sites via the Chief Financial Officer of the LHN.
None of these processes were practical within the scope of this evaluation. We therefore developed a proxy measure of each service’s budget, based on modelling assumptions, which we then compared to site Initiative revenues. Our approach involved the following steps:
Comparing the relative size of the Initiative MBS revenues to the modelled budget, expressed as a percentage.
The results of that analysis at a jurisdiction level are summarised in Table 4.7 (see next page) and indicate the following:
| Jurisdiction | Survey response Numbers (n) | MOdelled Salaries and wages (S&W) budget (total) | Aggregate Initiative MBS revenue, based on individual site receipts (2019‒20) for respondent sites | MBS Revenue as % of modelled salaries & Wages budget, at a jurisdiction level | MBS Revenues as a % of modelled S&W budget – Range of values within jurisdiction | |
|---|---|---|---|---|---|---|
| Smallest % for a respondent site within the jurisdiction | Largest % for a respondent site within the jurisdiction | |||||
| NSW | 21 | $59.628 m | $1.608 m | 3% | 0% | 7% |
| QLD | 7 | $24.317 m | $1.472 m | 6% | 0% | 80% (a) |
| WA | 11 | $61.654 m | $4.1 m | 7% | 1% | 82% (b) |
| NT | 5 | $15.728 m | $1.188 m | 8% | 4% | 38% |
| Total/measure for all respondent sites | 44 | $161.327 | $8.368 m | 6% | 0% | 82% |
| Other site aggregations | ||||||
| - Respondent sites in northern WA, NT and QLD | 22 | $98.272 m | $6.690 m | 8% | 0% | 82% |
| - Respondent sites in southern WA and NSW | 22 | $62.148 m | $1.679 m | 3% | 0% | 7% |
(a) Service with a very low reported FTE (1.7)
(b) Service with a very low reported FTE (0.4)
Importance of the Initiative to sustainability: normative assessment
The reason for the lesser level of support in WA is unclear, given the financial modelling suggests that revenue received under the Initiative is higher on average than in both NSW and Queensland.
Role of the Initiative in facilitating maintenance of core services
Assessments of the contribution of the Initiative to health service sustainability should be considered in the context of the assessment of the first program objective – enhanced access to primary care. In Section 4.1 we noted the Initiative has clearly improved. access to emergency medical care and after-hours services at many participating sites. The availability of financial resources underpins that service delivery development, evidence that the Initiative has contributed to delivery of these core services. However, it should be emphasised that access to the Initiative – and its associated support for primary care service development, access to greater levels of relevant healthcare workforce, and increased financial support – is not a guarantee of long-term health service viability. Historical service delivery arrangements, industrial arrangements and gradual population decline can all interact to threaten the sustainability of health services and compromise the models of care available to some small communities. The interaction of these various challenges is illustrated by our case study of the Nyngan MPS in north-western NSW (see Case Study Box #3 below).
We return to the issue of access to health services in outer rural and remote settings in our commentary on appropriateness of the Initiative in Section D of this chapter.
Development of sustainable health services: Summary assessment
Based on the analysis presented above, the evaluation team reached the following conclusions:
Section B: Program design & Administration
The evaluation brief specified that there should be an examination of the program’s design and administration. In this evaluation area, the team examined the Initiative’s eligibility criteria, administrative arrangements, including the MOU principles and objectives, required processes for stakeholder engagement and reporting, and Department of Health administrative arrangements.
Initiative eligibility criterion: Appropriateness
Stanthorpe Hospital: the need for a review process when site eligibility changes
Stanthorpe Hospital was granted an exemption under the Initiative in 2014 when the key eligibility criteria required a community to be <7,000 and in a District of Workforce Shortage. With the introduction of the MMM 5‒7 criteria, communities with populations above 5,000 people no longer satisfy that requirement. In 2020, the annual review of the MMM classification determined that Stanthorpe was an MMM 4 (rather than a MMM 5) and the Medical Director was advised that the site was no longer eligible and would have to cease MBS billing by 1 January 2022. While the Medical Director requested the Department to reconsider this determination, the event highlighted the absence of a review or appeal mechanism in the current MOU.
Initiative eligibility criteria: Summary assessment
Based on the analysis presented above, the evaluation team reached the following conclusions:
Development of a new MOU should consider introduction of mechanisms for dealing with the underlying service development needs of sites that no longer comply with the MMM 5 to 7 eligibility criterion. This could include PHN support for innovative RG models.
Suitability of current administrative arrangements
Principles: Value and contribution
MOU Principles: Summary assessment
The current MOU principles have minimal impact on the Initiative’s operations. However, they do provide a useful statement of the context explaining why the Initiative was introduced in 2008 and continues to operate. It may be better that these general statements are rephrased as a ‘preamble’ in a redrafted MOU. The current statement relating to engagement with primary care practitioners has ongoing importance in informing applications and consultation processes once participation of a site is approved; it should be retained in the operational arrangements of the MOU.
Site engagement of stakeholders
The guidelines indicate that sites should engage with local stakeholders for the purpose of operational planning as a component of the application process. The application requires signed endorsement by local GPs, hospital doctors, ACCHOs, and the RFDS that may be materially affected by the Initiative, together with other stakeholders including the PHN, local government and community representative.
Across sites, engagement with RWAs to identify workforce priorities and workforce development opportunities was very limited or absent. Similarly, there was limited formal engagement with PHNs to utilise their health needs assessment for reinvestment considerations, or alignment of reinvestment with PHN commissioning opportunities. PHNs and RWA consultations identified opportunities to better maximise benefits derived from the Initiative through collaborative planning and leveraging available funds and programs.
External stakeholders identified concerns with transparency of the program. Stakeholders indicated difficulty in obtaining a copy of the MOU between the Commonwealth and Queensland, whereas the MOUs between the Commonwealth, NSW and WA are available on the internet. Issues were also raised about apparent absence of a review of operational plans on a regular cycle (e.g., at the commencement of each MOU) or mechanism to trigger the review of the eligibility of a site where local service status changed.
The Murrumbidgee LHD (MLHD) has 22 facilities that hold an Initiative Exemption, of which 11 are an MPS and 11 are hospitals. Medical services in these facilities are predominantly provided by GP VMOs. MLHD operates the Remote Medical Consultation Service (RMCS) to support clinicians in outlying hospitals by prescribing medical treatments, providing first aid advice and identifying when further care is required. Sometimes hospitals in outlying areas are not staffed by doctors all the time. In such instances the RMCS allows clinicians (usually nursing staff) to seek advice on appropriate treatment options and have patients assessed via phone or video link to avoid admitting or transporting patients long distances unnecessarily. The MLHD currently has a contract with Rural and Remote Medical Services (RARMS) to provide telehealth support to rural facilities for category 4 and 5 presentations when there is not a doctor on-call to the hospital.
The Manager of Revenue Performance & Improvement sits in the Finance and Performance section of the MLHD and has the responsibility of managing the Initiative across all rural facilities. This position supports each site in the application and operational planning process and convenes bi-monthly meetings of the local Initiative committee to review implementation issues and plan for reinvestment of funds. The Manager also supports sites to develop, implement and review Medicare claiming processes and works with the practices and LHD Medical Administration to arrange VMO contracts, streamline applications for provider numbers for VMOs and GP registrars, provide information packs for new doctors including consent to opt into the Initiative and opt into gap cover arrangements. The Manager shares ideas about reinvestment opportunities across sites and prepares site level revenue and expenditure reports that are visible to local stakeholders. The Manager works strategically with the Ministry of Health to provide information about the Initiative and value of reinvestment to communities.
- Workforce development to address service gaps: training for a local GP in pain management and equipment for ultrasound guided injections. This training will enable local access to pain management services and the trained GP will provide training to other GPs to increase capacity across the region.
- Workforce for delivery primary healthcare: Nurse Practitioner (Gundagai Medical Centre); Mental health nurse (Gundagai Medical Centre); short-term allocation of hours for a trauma counsellor to work from the Temora Medical Centre.
Engagement with stakeholders: Summary assessment
Greater transparency about funds available for reinvestment in a town could be enhanced by insights of other stakeholders about underlying health needs in their community. In addition to GPs and community members, this could include RWA, PHN, local ACCHO or State Affiliate representation.
The evaluation team observed examples of innovation which had occurred because of LHNs engaging with a broader range of stakeholders around Initiative implementation plans. One LHN developed links with universities, general practice training providers and larger regional hospitals to progress junior doctor training across hospitals and general practice. Some locations used the Initiative to extend GP services to smaller MMM 5‒7 communities beyond their immediate town, e.g. Stanthorpe, Longreach, Tully.
Reporting arrangements
Reporting arrangements: Summary assessment
Sub-regional and jurisdiction governance
NACCHO’s written submission to the evaluation indicated there was inadequate consultation with the sector at the local ACCHO level and with their jurisdiction affiliates in relation to new applications, ongoing implementation of the Initiative and reinvestment. RDAA raised concerns around the governance of reinvestment, highlighting the risk of funding generated through the Initiative being re-directed to the bottom line of public hospital bodies rather than used to increase access to primary care services as intended. While it was acknowledged that the Initiative is an excellent mechanism to use when there is market failure in community based general practice and other primary care models, it should be directed to supporting the jurisdictions to develop integrated models of care. This was re-iterated by several PHNs. Furthermore, PHNs have capability in developing primary healthcare models of care and patient information system support that the hospitals could draw upon.
CASE STUDY BOX # 6
Under the current MOU, it is the intent that revenue is reinvested at the site (according to plans set out in the Operational Plan) and overseen by a local governance group. As outlined immediately above and in earlier sections, there is considerable variability between and within jurisdiction in local governance processes. There were a number of external stakeholders who identified opportunities to use a S19(2) exemption to support system change (e.g. the Murrumbidgee single employer model for Rural Generalist trainees employed by the LHD and based in general practice) or address structural issues particularly at a sub‑regional level, e.g. the 4Ts model. This was seen to have potential for greater benefit particularly where the quantum of investment required per site was relatively modest, or where smaller communities did not have a doctor (but had primary care needs) and could not derive financial benefit from an exemption.
CASE STUDY BOX # 7
This one-employer model seeks to integrate multidisciplinary care across primary and acute care services in small rural communities. It differs to other single-employer models in that it includes nursing and administrative staff as well the GPs. It is anticipated that pooled resourcing will sustain more comprehensive health services in communities than may otherwise have been the case. While Western NSW LHD is placed as the single employer across these towns, the project does not assume that the LHD should be the single employer if this model were to be translated more broadly across other communities at some future time.
This example demonstrates the potential benefit that can be realised through collaborative planning and resourcing across primary and secondary care settings at a sub-regional level.
A sub-regional governance group that includes representation from the LHN, PHN, RWA, local ACCHO and local government enables access to relevant health and workforce needs assessment to inform prioritisation and planning, provides the foundation for collaborative resourcing to maximise the potential benefit of the Initiative, can identify changes within the service system that may need to be considered in relation to the operation of the Initiative (e.g. new private practice that may wish to establish, nuanced negotiation of Medicare items to be claimed) and provide transparency to local, sub-regional and regional stakeholders internal and external to the LHN for planning and implementation of the Initiative.
Sub-regional and jurisdiction governance: Summary assessment
Based on the analysis presented above, the evaluation team reached the following conclusions:
Department of Health administration
Department of Health administration: Summary assessment
The current reporting mechanisms of the Initiative focus on levels of MBS revenue generation. Appreciation of the models of care and closer examination of reinvestment processes at each site would enhance understanding of underlying drivers for the MBS billing.
efficiency of current arrangements
MBS billing – site & LHN processes
transfer case details from the hospital patient administration system and ED clinical management system (where treating doctors recorded their notes about the nature of their clinical intervention) into the Medicare billing system
allocate an MBS item number, and
too busy in ED
had limited interest or incentive to bill where they were already paid under state awards or VMO arrangements
limited sharing of information between LHNs within some jurisdictions (NSW and Queensland) to develop improved administrative processes, i.e. each site has developed their own approach to collecting data and checking claim veracity
variation between sites in requesting/requiring patients to sign bulk bill claims forms (DB4); the requirement to sign had been waived due to COVID-19 but it was unclear how long this would continue, and
The case study analysis identified relatively large levels of administrative staff associated with the Initiative, ranging from 0.5 FTE to 2.2 FTE per site. The administrative staff, in addition to supporting the claims management processes, would assist with reception duties and patient flow management (e.g. queuing in the waiting room).
The NT health services sought to deal with the administrative complexity by providing support to all service delivery sites operating a S19(2) exemption. Each health service (Top End and Central Australia) had a billing support team that trained new doctors and revenue clerks in MBS billing processes, reviewed claims and lodged them on behalf of the site and ensured that all new doctors received their prescriber numbers from Services Australia in a timely manner. These arrangements in the NT reflected:
The evaluation team undertook a sample survey (n=8) in two jurisdictions of the reasons that some sites listed on the Department as participating had not billed in the previous financial year (2019–20). These reasons included: variation in the local model of care (n=2) e.g. where the GP had changed their preference for where they consulted with patients (from the hospital to private practice); the status of the facility had changed from a hospital to a community health service (n=1); delivery arrangements at the hospital had changed to a contracted provider from outside the town (n=6); and the non-reporting of revenue was a data extraction error by the LHN in the data submitted to the Department (n=1).
MBS billing arrangements: Summary assessment
Based on the analysis presented above, the evaluation team reached the following conclusions:
MBS claim levels not linked to underlying population need
Overall revenue derived from the Initiative was $13.6 m in 2019–20 across the 92 billing sites in that financial year. However, there was a wide variation in the quantum of Medicare billing generated by different sites.
In 2019–20 eight sites generated over $600,000 in revenue each (ranging from $0.600 million (Fitzroy Crossing) to $1.043 million (Derby)).
This analysis highlights that revenue generating capacity under the Initiative is typically linked to the number of salaried doctors at a site, especially where there are larger emergency departments – as in the bigger MMM 5 to 7 towns in WA, NT and Queensland.
The models of care that operate within the context of the GP VMO arrangements (as in NSW) generate relatively less MBS revenue for their sites under the Initiative, because the doctors are not salaried and operating extended hours or 24-hour emergency departments (as in Queensland and the Northern Territory).
Link of Initiative to underlying population need: Summary assessment
Funding contributions to different sites resulting from the Initiative can be internally inequitable within the program arrangements – larger sites with more salaried doctors have a greater ability to undertake MBS billing. This characteristic highlights a program design characteristic of the Initiative; MBS revenues of a site are not directly linked to underlying health needs of a community. There is limited capacity to address this program characteristic – the foundation of the Initiative is primarily as a top-up to funding, enabled by access to MBS billing. Communities and health service providers need to access other funding sources to address local healthcare needs in a more targeted way, including programs administered or commissioned by PHNs, RWAs, aged care funding, and locally based service delivered by local providers such as local government and LHNs.
Ongoing barriers to care
The concept of access to healthcare can be described as the potential ease with which consumers can obtain healthcare. Access in a healthcare context is a complex and multidimensional concept. Disaggregation of the concept into a range of dimensions is outlined in Table 4.9. This more granular description allows policy makers and health service organisations to identify key questions to be addressed in the planning and delivery of services to ensure optimal access to healthcare for Australians living in regional, rural and remote areas.
| Access dimensions | Definitions | |
|---|---|---|
| Health system characteristics | Population characteristics | |
| Availability | Volume and type of services | Volume and type of service the population needs |
| Geography | Proximity of providers to consumers | Ease with which the population can transcend this space |
| Affordability | Direct and indirect costs of securing healthcare | Consumers’ ability to meet the direct and indirect costs of healthcare |
| Accommodation | Manner in which the supply resources are organised | Consumers’ ability to contact, gain entry to and navigate the health system |
| Timeliness | Time until healthcare can be provided | Urgency of the need for healthcare |
| Acceptability | Providers’ attitudes and beliefs about health and personal characteristics of consumers (e.g. age, gender, ethnicity, religion) | Consumers’ attitudes and beliefs about health and personal and practice characteristics of providers |
| Awareness | Communication of health and health systems information to consumers | Consumers’ understanding of their health needs and knowledge of how to have these needs met |
Legend: Evaluative Assessment Colour Code: impact of the Initiative on accessibility dimensions (as specified in Table 4.9) at each of the case study sites
| All sites | Many sites [5 to 10 sites] | Some sites [1 to 4 sites] |
|---|
CASE STUDY BOX # 9
Mamu Aboriginal Health Service is based in Innisfail and provides outreach services to Tully, Babinda and Ravenshoe. A GP services the Tully community one day per week. However, Mamu is experiencing difficulties recruiting doctors.
Tully Hospital is staffed by eight doctors. This includes three permanent SMO appointments, four PHOs (two rotating from Cairns Hospital and two rotating from Innisfail Hospital) and one SMO (temporary appointment) funded through Initiative revenue. Tully Hospital is currently funded for nine acute care beds but can operate up to 20 beds (if funded).
- Timeliness: (1) there is a six to eight week wait for appointment with GP fellow at private practice, two weeks for GP registrars; two-week wait at Tully GP clinic; and the solo practice at Mission Beach has closed books
- Systems to support quality primary healthcare: while Tully Hospital GP Clinic has River Medical – (Communicare) in place, systems have not yet been operationalised to support health assessments and care plans. This is a focus of future work.
Ongoing barriers to care: Summary assessment
Based on the analysis presented above, the evaluation team reached the following conclusions:
The Initiative program design – with its reliance on MBS billing to determine the level of top-up revenue to a site – does not vary resourcing according to a range of other underlying access problems encountered by communities residing in outer rural and remote areas; the mix of these problems is highly variable by site and relates to service availability of primary care services other than emergency care, geographic proximity to services, affordability, system navigation by patients, cultural acceptability, and health literacy.
Effectiveness
With respect to effectiveness in meeting overall objectives, we found that the Initiative improved access to urgent medical care and after-hours services at a large proportion of participating sites. It has also contributed to increased availability of primary care services in many locations. Much of the MBS revenue reinvestment was allocated to medical officer remuneration to support acute hospital emergency services.
Nationally MBS revenues under the Initiative represented in the order of 6% of modelled salaries and wages of participating sites, suggesting that the Initiative is, on average, a reasonably significant contributor to overall revenue of these sites. This proportion varied significantly by both site and jurisdiction.
Program design and administration
Appropriateness
The way forward: Options for program refinement
The findings from the evaluation suggest that changes to the current arrangements should be considered to ensure implementation of the Initiative:
is responsive to the context in which it is operating
Overview of options
There is variation in governance and administration of the Initiative between jurisdictions, as well as between LHNs within jurisdictions. External stakeholders identified the need for greater transparency in all aspects of the Initiative from application and operational planning to reinvestment decisions, facilitated by establishing a cycle of planning and review.
While the Initiative presents a revenue stream to local health services, the median quantum of MBS available for reinvestment available at a community level is relatively modest in the majority of sites. Partnering with local, regional or state-level agencies offers opportunities for joint planning, resource allocation and investment to maximise benefit derived from the Initiative.
Option 2 (b): a Commonwealth/jurisdiction bi-lateral governance committee (one for each participating jurisdiction)
Establishing mechanisms to maximise benefit to communities through collaborative planning and co-investment by exploring the relationship with other Commonwealth and jurisdiction program investments in the town and its surrounding community (Option 3), and
Place based planning and service development.
These options were beyond the scope of this evaluation, which was to focus on the effectiveness, program rules and appropriateness of the Initiative.
Option 1: Administrative refinement of the Initiative
Priorities for reinvestment in primary health care should be informed by local health and workforce needs assessment
The Initiative seeks to promotes the development of a local health workforce skilled to work in rural and remote communities
promote the provision of urgent medical care where access to this care is limited
expand the availability of comprehensive team based primary care in rural and remote communities
Option 2: Revise program governance arrangements
To facilitate this enhanced governance, we suggest a requirement for all sites to implement an organised structure of sub-regional stakeholders proximate to a site with representation from:
LHD executive
A community representative.
This sub-regional governance group would have responsibility to assess:
review reports prior to submission to the jurisdiction.
The sub-regional governance committee should meet at least six monthly, with secretariat support provided by the LHN.
Community representative
Other local health services (private providers, ACCHO)
| Benefits of Option 2(a) |
|---|
|
Any changes in broader health policies that may impact on the operation of the Initiative
Jurisdictions can inform the Commonwealth of changes in the status of participating sites that may affect:
The jurisdiction governance committee should meet at least once within each financial year of the MOU operation, ideally around the middle of the year, to progress consideration of new applications.
Option 3: Use sub-regional governance committees as a coordination mechanism
after-hours arrangements
mental health programs, and
| Benefits of Option 3 |
|---|
In addition to benefits identified for Option 2 (a), this extension to sub-regional governance would ensure that:
|
Option 4: Administrative refinement to program processes
Option 4(a): Periodic refresh of operational plans
Scope and rationale: sites should be required to update the operational plan at least once an MOU cycle (at present the majority of sites are operating on plans that were cleared at the time of their original application, between 2008 and 2015).
Option 4(b): Processes for dealing with changes to site eligibility where a site no longer meets the eligibility criterion of being located in MMM 5 to 7
Scope and rationale: The current MOU contains no review mechanism to assess the impacts of removing a site’s entitlement to participate in the Initiative. A transparent review process for sites that no longer meet the eligibility criterion would be welcomed if it could ensure ongoing stability in service delivery access. We suggest a structured review process to deal with such circumstances:
The review report could be submitted to the sub-regional governance committee proposed in Option 2(a).
If there is ongoing support locally from the sub-regional governance committee, the review report could then be forwarded to the Commonwealth / jurisdiction committee proposed in Option 2(b). This would examine state or territory commitments to maintain and/or expand their contribution to the service, so that the scope of the Commonwealth role does not drift beyond facilitating access to MBS funding.
| Benefits of Option 4(b) |
|---|
Scope and rationale: at present extensive effort is involved in preparing local patient consent forms, check lists for in-scope MBS items, and application forms and processes for new registered provider numbers. New and existing sites are often unclear whether particular types of expenditure meet the reinvestment rules of the program.
An on-line clearing-house could be developed to store these materials and curate responses to site queries. One jurisdiction could be asked to support this on-line function on behalf of all participating jurisdictions.
Understanding of how the MBS funds are being used at a site level would be enhanced if submission and storage of annual report data were enabled by an online portal linked to a database to facilitate data management. Sites could enter their data online and edit this data up to the 31 August close-off. The database should contain links to the Operating Plan. Submissions should be required to explain how the reinvestment is in alignment with the Operating Plan or varies from the Plan.
The Commonwealth program area should produce annual reports on how the MBS funds have been reinvested at a site and jurisdiction level. This information could be shared with jurisdiction and sub-regional committees.
| Benefits of Option 4(d) |
|---|
Appendices
Detailed evaluation questions specified in the RFQ
Does the Section 19(2) Initiative continue to meet the need to improve access to primary care in rural and remote areas?
To what extent does this Program still contribute to resolving this issue?
Should the eligibility criteria be modified and if so, how should it be changed?
Are the current administrative arrangements and processes appropriate for management, accountability and transparency purposes and if not, how can these be improved?
Are the Department of Health administrative processes in terms of application assessment, approval, ongoing management and reporting adequate for review purposes?
The effectiveness of the program. Within this area the RFQ states that the detailed evaluation questions to be answered are:
Has the funding improved the provision and consistency of primary care initiatives at the sites and in what areas is it reinvested?
Has there been an increase in primary healthcare community health programs in this location, and if so, can this be attributed to the Section 19(2) Initiative?
List of other S19(2) Exemption sites
S19(2) Exemptions Initiative in New South Wales
S19(2) Exemptions Initiative in Queensland
| Categories of S19(2) Exemption, by Service / Location | ||||
|---|---|---|---|---|
| COAG | ACCHO | Indigenous Health | Murrumbidgee | RVTS |
Babinda Hospital Boulia PHC Capella OC Collinsville Hospital Dimbulah PHC Gin Gin Hospital Hughenden HC Jundah PHC Longreach Hospital Monto HS Mossman MPS Proserpine Hospital and CHC Quilpie MPS Tambo PHC Tara Hospital Winton MPS |
Aboriginal and Torres Strait Islander Community Health Service Brisbane Ltd, Woolloongabba Carbal Medical Services, Toowoomba Charleville and Western Areas Aboriginal and Torres Strait Islander Community Health Limited, Charleville Goolburri Aboriginal Health Advancement Corporation, Toowoomba Goondir Health Service, Dalby Kalwun Health Service, Miami Kambu Aboriginal and Torres Strait Islander Corporation for Health, Ipswich Service, Mareeba Nhulundu Health Service, Gladstone Wuchopperen Health Service Ltd, Manoora Yulu-Burri-Ba Aboriginal Corporation for Community Health, Dunwich |
Dauan Island Erub (Darnley) Island Mer Island Moa (St Pauls) Island Waiben (Thursday) Island Warraber Island Aurukun Coen Lockhart River Mapoon Jumbun Yarrabah The Southern Queensland Centre of Excellence in Aboriginal and Torres Strait Islander Primary Health Care, lnala Palm Island Burketown Julia Creek Karumba |
Mt Isa – Gidgee Healing |
|
S19(2) Exemptions Initiative in Western Australia
S19(2) Exemptions Initiative in the Northern Territory
| Categories of S19(2) Exemption, by Service / Location | ||||
|---|---|---|---|---|
| COAG | ACCHO | Indigenous Health | Murrumbidgee | RVTS |
Adelaide River HC Batchelor HC Yulara HS |
Ampilatwatja Health Centre Aboriginal Corporation, Ampilatwatja Community Katherine West Health Board Aboriginal Corporation, Katherine Laynhapuy Homelands Aboriginal Corporation, Yirrkala Nganampa Health Council Inc, Alice Springs Pintupi Homelands Health Service, Kintore |
Maningrida CHC Minjilang (Croker Island) CHC Wadeye (Port Keats) CHC Warruwi (Goulburn Is) CHC Robinson River CHC Alyangula (Groote Eylandt) HC Milyakburra (Bickerton Is) CHC Umbakumba CHC Atitjere (Harts Range) CHC Bonya (Baikal Bonja) CHC Laramba (Napperby) CHC Ntaria (Hermannsburg) CHC Tara (Neutral Junction) CHC Ti Tree CHC Wilora (Stirling) CHC Wirilyatjarrayi (Willowra) HC Canteen Creek (Orwatijilla) HC Elliott CHC Julanimawu Milikapiti HC |
||
S19(2) Exemptions Initiative in South Australia, Victoria, Tasmania and Australian Capital Territory
Australian Government programs targeting development of the rural workforce
| Year | Policy | Focus | Strategy and Activities |
|---|---|---|---|
| 1997 and ongoing | Rural Health Multidisciplinary Training Program – previously the University Department of Rural Health Program and the Rural Clinical Training Support Program | To provide infrastructure and academic network in regional, rural and remote areas to improve the distribution of the health workforce through the delivery of rural training experience. | 16 UDRHs and 19 RCSs establish and maintain networks of rural clinical supervisors and placements to expose undergraduate medical and health professional students to rurally based clinical training and practice to promote interest in, and uptake of, a rural health career. |
| 2016 | Rural Locum Assistance Program funded under the Health Workforce Program – administered by Aspen Medical since April 2016 with an annual appropriation of around $11.5 million (currently to June 2022). | To enhance ability of specialists (obstetrics and anaesthetics), procedural GPs, nurses and allied health professionals in rural Australia to undertake leave for recreation or to undertake continuing professional development. | Supports eligible rural health professionals to access CPD or take leave, metro-based GPs to upskill in emergency medicine to better prepare for rural locum work, and urban based health professionals to experience rural practice by undertaking a locum. |
| 2017 | Health Workforce Scholarship Program | To increase access to health services in rural and remote areas where there is skill shortage. This program replaced a number of scholarship programs including Nursing and Allied Health Scholarship Support Scheme and Rural Australian Medical Undergraduate Scheme. |
Provides bursaries and scholarships to existing health professionals committed to rural service. RWA administer program ($33 m over three years to June 2020) to deliver HWSP in MMM 3–7. Informed by the RWA’s Health Workforce Needs Assessment. |
| 2017 | Rural Workforce Support Activity – Go Rural | Grow the sustainability and supply of the health workforce. | RWAs engaging with Rural Health Clubs to promote careers to rural secondary school students; university student rural immersion activities; Supporting clinical placements for nursing and allied health students; linking students with mentors to guide rural journey. |
| 2018 | John Flynn Prevocational Doctor Program (JFPDP) – announced as part of the 2021-22 Federal Budget | The JFPDP will commence from 1 January 2023 and will consolidate the two funding streams (core and Rural Generalist) under the Rural Junior Doctor Training Innovation Fund (RJDTIF). The RJDTIF arrangements will continue until 31 December 2022. JFPDP will expand the number of rural primary care rotations available each year and increase rural primary care rotations for hospital-based prevocational doctors (Postgraduate Year 1-5) in rural areas. | |
| 2018 | Stronger Rural Health Strategy – Bonded Medical Programs (reformed). | Aim of the reform is greater flexibility and more support for bonded doctors and better target return of service to underserviced areas in most need. | From 1 January 2020, participants of Bonded Medical Program can complete Return of Service Obligation through working in eligible location in MMM 2–6, Distribution Priority Areas (DPA) for GPs areas, outer Metro and Districts of Workforce Shortages for the participants chosen specialty. |
| 2018 | Nursing in Primary Health Care (NiPHC) Murray-Darling Medical Schools Network |
||
| 2018 | Stronger Rural Health Strategy – Support for Aboriginal and Torres Strait Islander Health Professional Organisations | This aims to build and support the Aboriginal and Torres Strait Islander health workforce and continue to increase the cultural capability of the broader health workforce to better meet the needs of Aboriginal and Torres Strait Islander people. | This initiative funds a variety of activities, including training, mentoring, support, and activities to promote health careers to Aboriginal and Torres Strait Islander people. |
| 2018 | More Doctors for Rural Australia Program (MDRAP) | The MDRAP is a workforce program designed to support non-vocationally recognised (non-VR) doctors to deliver general practice services in rural and remote Australia and prepares them to join a formal fellowship pathway. Overseas and Australian trained doctors are eligible to join the MDRAP. | Non vocationally registered doctors participating in the program will be able to access a Medicare benefit while working toward entry to a fellowship program. |
| 2018 | National Rural (Medical) Generalist Pathway | To improve workforce supply by coordinating the training pipeline for rural generalists to deliver quality healthcare in rural, remote and regional communities (focusing on MMM 3‒7) | Facilitate a coordinated and efficient medical training pathway with nationally recognised skills. Establish or expand coordination units within each jurisdiction to bridge the gap between national objectives and regional programs. Expansion of the Rural Junior Doctor Training Innovation Fund (RJDTIF) will support the pathway. The Commonwealth has provided funding for 100 RG GP training positions commencing 2021. These will be delivered through the Australian College of Rural and Remote Medicine (ACRRM) Rural Generalist Training Scheme (RGTS). |
| 2020 | To extend the Allied Health Rural Generalist training pathway to non-government organisations and private practices working in aged care, disability and primary healthcare. . |
||
| 2018 | Remote Health Workforce Education, Support & Professional Services Program | Support to health professionals working in remote areas, or other circumstances of professional isolation, with education, mental health and well-being support, and professional services that are relevant to their context of practice. | Supports the provision of: relevant education, training and professional development opportunities for health professionals working in remote and isolated areas of Australia; mental health and wellbeing support to remote healthcare professionals (and their families); and professional services contributing to the recruitment and retention of a stable remote health workforce. |
List of stakeholders consulted
Table 6.3: Stakeholders consulted – Departmental, RWA and peak bodies
| STATE | NAME | TITLE | ORG/DEPARTMENT/AREA |
|---|---|---|---|
| Internal contacts, Department of Health | |||
| Sandra Downie | Assistant Director | Health Care Homes Governance, Reporting and Engagement Section | |
| Alan Stephen | Departmental Officer | Health Care Homes Governance, Reporting and Engagement Section | |
| James Newhouse | Assistant Director | Geospatial and Hospital Analytics - HERD | |
| Loc Thai | Director | Geospatial and Hospital Analytics - HERD | |
| Emma Rowland | Assistant Director | Primary Health Care Policy Section, Indigenous Health Division | |
| Tony Lawrence | Assistant Director | MBS Analytics SN | |
| David Nott | Director | Provider Benefits Integrity and Digital Health Division - Director, Public Hospital Compliance Section, Compliance Audit and Education Branch | |
| Rohan Sanders | Departmental Officer | Provider Benefits Integrity | |
| Michael Ryan | Director | Diagnostic Imaging Section, Diagnostic Imaging and Pathology Branch, Medical Benefits Division | |
| Fifine Cahill (with Louise Larcon) | Assistant Secretary | National Health Reform Branch | |
| Professor Ruth Stewart | National Rural Health Commissioner | NHRC | |
| Gayle Nicholson | Senior Policy Officer | Medicare Providers, Services Australia | |
| Emma Phelan (written comments) | Director | Health Training Branch, HWA | |
| Tino Rizzo | Acting Director | GP Systems, Health Training Branch (Single Employer Trials) | |
| Louise Clarke | Assistant Secretary | Rural Access Branch, HWA | |
| Kathryn Yuile | Director | Health Workforce Strategic Policy Section, Health Workforce Reform Branch | |
| Jurisdictions | |||
| NSW | Josephine Hull | Senior Policy Officer | Strategic Reform and Planning Branch |
| NSW | Michelle Maxwell | Director, Strategic Change | Strategic Reform and Planning Branch |
| NSW | Samantha Reid | – | – |
| NT | Anthony Burton | Director | Intergovernmental Relations and Ageing |
| NT | Melissa Brooke | – | – |
| NT | Maja Van Bruggen | Director, Revenue Management | – |
| WA | James Thomas | Executive Director | Health Programs WACHS |
| WA | Anna McDonald | Project Coordinator | Health Programs WACHS |
| QLD | Ricky Barker | Principal Advisor | Revenue Strategy and Support Unit, Queensland Health |
| QLD | Karie Karvourn | – | Office of Rural Health |
| Non-participating jurisdictions | |||
| SA | Katie Bourke, Skye Jacobi, Hendrika Meyer | Principal Policy Officer | Strategy and Intergovernment Relations |
| SA | Chris McGowan | Chief Executive | Department for Health and Wellbeing |
| Potential new States and Territories | |||
| VIC | Kate Boucher | Principal Policy Advisor /Allied Health Workforce | Health Workforce Policy |
| VIC | Nicola Farray | Director Commissioning and System Improvement | Victorian Department of Health |
| VIC | Catherine Harmer | Manager Rural Policy | Victorian Department of Health |
| VIC | Praveen Sharma | Project Director Healthcare Worker Protections | Medical Workforce |
| TAS | Rebekah Moore | N/A | Government Relations and Strategic Policy |
| TAS | Erin Taylor | Branch Manager | Government Relations and Strategic Policy |
| Rural workforce agencies | |||
| QLD | Chris Mitchell | Chief Executive Officer | Health Workforce |
| WA | Tim Shackleton | Chief Executive Officer | Rural Health Workforce |
| WA | Kelli Porter | General Manager | Workforce - Rural Health Workforce |
| NT | Heather Keighley | – | Northern Territory PHN - Workforce |
| NT | Paul Connolly | – | Northern Territory PHN |
| NT | Robin Moore | Executive Director | Northern Territory PHN - Workforce |
| SA | Lyn Poole | Chief Executive Officer | Rural Doctors Workforce Agency |
| NSW | Richard Colbran | Chief Executive Officer | Rural Doctors Network |
| NSW | Michael Edwards | Policy Officer | Rural Doctors Network |
| Peak bodies | |||
| Pat Turner | Chief Executive Officer | NACCHO [written submissions requested] | |
| Peta Rutherford | Chief Executive Officer | Rural Doctors Association [discussion and written submissions received 31 May 2021] | |
Appendix E MBS claims – framework for aggregating individual items
Definitions of the item categorisation used to derive aggregated items used in the MBS data analysis are given in Table 6.5.
| S19(2) MBS Item aggregated category | MBS groups / subgroups | Associated variables |
|---|---|---|
| ‘Non-Referred Attendances, ‘NRA’ (A/hrs and EPC to be separated out but retained as aggregated sub-category)’ | GROUP(S) A01, A02, A05, A06, A07, A11, A14, A17, A18, A19, A20, A22, A23, A27, A30, A34, A35, A39, A41, SUBGROUP(S) A1501, A3601, A3604, A4001, A4002, A4003, A4010, A4011, A4012, A4013, A4014, A4015, A4016, A4019, A4020, A4021, A4022, A4027, A4028, A4029, A4030, ITEM(S) 5021, 5022, 5027, 5030, 5031, 5032, 5033, 5035, 5036, 5042, 5044, 735, 739, 743, 747, 750, 758, 90264, 90265, 92170, 92171, 92176, 92177 | Jurisdiction |
| Date of service provision | ||
| Service location | ||
| Non-referred attendances ‒ Practice Nurse | GROUP(S) M12, SUBGROUP(S) M1823, M1824 | |
| Other Allied Health | GROUP(S) M03, M06, M07, M08, M09, M10, M11, M15, M16, M17, M25, M26, SUBGROUP(S) M1801, M1802, M1803, M1804, M1806, M1807, M1808, M1809, M1811, M1812, M1813, M1814, M1815, M1816, M1817, M1818, M1819, M1820, M1821, M1822, M1825, M1826 | |
| Specialist attendances | GROUP(S) A03, A04, A08, A09, A12, A13, A24, A26, A28, A29, A31, A32, A33, T06, SUBGROUP(S) A3602, A4004, A4005, A4006, A4007, A4008, A4009, A4017, A4018, A4023, A4024, A4031, A4032, A4033, A4034, A4035, A4036, A4037, A4038, ITEM(S) 5001, 5004, 5011, 5012, 5013, 5014, 5016, 5017, 5019, 5039, 5041, 820, 822, 823, 825, 826, 828, 830, 832, 834, 835, 837, 838, 855, 857, 858, 861, 864, 866, 871, 872, 880, 90266, 90267, 90268, 90269, 92172, 92173, 92178, 92179 | |
| Obstetrics | GROUP(S) T04 | |
| Anaesthetics | GROUP(S) T07, T10 | |
| Pathology | ||
| Diagnostic Imaging | GROUP(S) I01, I02, I03, I04, I05, I06 | |
| Operations | GROUP(S) T08 | |
| Radiotherapy and Therapeutic Nuclear Medicine | GROUP(S) T02, T03 | |
| Other MBS services | GROUP(S) C01, C02, C03, D01, D02, M01, M13, M19, O01, O02, O03, O04, O05, O06, O07, O08, O09, O11, T01, T11 | |
| Nurse Practitioners | Group M14, SUBGROUP(S) M1805, M1810 | |
| After Hours Non-Referred Attendances | Identified as separate sub-categories of items. | |
| Enhanced Primary Care |
Appendix F MBS benefits paid under the Initiative, 2019–20, by jurisdiction & aggregated category
Table 6.7: QLD MBS benefits paid by aggregated MBS categories of all participating sites (n=39)
| MBS Aggregated Categories | Total claims for all sites | Percent of total for all sites | Mean claims per site ($) | Median claims, per site ($) | Range of values, all sites (min and max) | No. of sites with zero claims |
|---|---|---|---|---|---|---|
| 1. Non-referred Attendance(sub-total) – common items (e.g. 3, 23, 36, 44) | $2,698,422 | 50.1% | $69,190 | $23,197 | $0–$430,238 | 1 |
| 2. After-hours Non-referred Attendance – common items (sub-total) | $1,474,463 | 27.5% | $38,096 | $20,315 | $0–$295,586 | 5 |
| 3 Assessment related items, including disease management and other primary care professionals (sub-total) | $113,454 | 2.2% | $905 | $0 | $0–$41,282 | |
| $11,029 | 0.2% | $703 | $0 | $0–$5,191 | 31 | |
| $31,729 | 0.6% | $1,233 | $0 | $0–$17,453 | 30 | |
| $14,262 | 0.3% | $786 | $0 | $0–$3,059 | 20 | |
| $52,392 | 1.0% | $1,763 | $0 | $0–$41,282 | 29 | |
|
$1,175 | 0.0% | $450 | $0 | $0–$1,053 | 34 |
|
$2,867 | 0.1% | $493 | $0 | $0–$2,744 | 35 |
| 4. Other MBS items (sub-total) | $1,352,604 | 20.2% | $4,371 | $0 | $0–$102,187 | |
| $3,087 | 0.1% | $499 | $0 | $0–$1,462 | 32 | |
| $8,827 | 0.2% | $645 | $26 | $0–$6,331 | 11 | |
| $38,877 | 0.7% | $1,417 | $0 | $0–$20,532 | 33 | |
| $265,345 | 4.9% | $7,188 | $3,235 | $0–$63,635 | 1 | |
|
$89,620 | 1.7% | $2,718 | $0 | $0–$43,103 | 26 |
|
$90,751 | 1.7% | $2,747 | $0 | $0–$45,950 | 34 |
| $586,097 | 10.9% | $15,383 | $4,908 | $0–$102,187 | 1 | |
| Total | $5,369,118 | 100% | $137,437 | $55,366 | $8,024–$968,524 |
| MBS Aggregated Categories | Total claims for all sites | Percent of total for all sites | Mean claims per site ($) | Median claims, per site ($) | Range of values, all sites (min and max) | No. of sites with zero claims |
|---|---|---|---|---|---|---|
| 1. Non-referred Attendance) – common items (e.g. 3, 23, 36, 44) | $1,219,613 | 58.6% | $203,269 | $150,224 | $37,725–$565,240 | 0 |
| 2. After-hours Non-referred Attendance | $350,727 | 16.8% | $58,454 | $337 | $0–$217,641 | 3 |
| 3. Assessment related items, including disease management and other primary care professionals (sub-total) | $191,860 | 9.3% | $5,329 | $154 | $0–$32,656 | |
|
$56,785 | 2.7% | $9,464 | $7,329 | $0–$32,656 | 1 |
|
$90,973 | 4.4% | $15,162 | $17,193 | $0–$29,456 | 2 |
| $18,857 | 0.9% | $3,143 | $2,781 | $93–$6,480 | 0 | |
| $1,221 | 0.1% | $203 | $0 | $0–$1,221 | 5 | |
| $24,024 | 1.2% | $4,004 | $1,764 | $0–$13,740 | 2 | |
| $0 | 0.0% | $0 | $0 | $0–$0 | 6 | |
| 4. Other MBS items (sub-total) | $319,731 | 15.4% | $7,613 | $1,318 | $0–$74,325 | |
|
$800 | 0.0% | $133 | $0 | $0–$585 | 4 |
|
$36,764 | 1.8% | $6,127 | $7,256 | $559–$10,064 | 0 |
| $0 | 0.0% | $0 | $0 | $0–$0 | 6 | |
| $53,359 | 2.6% | $8,893 | $2,275 | $1,034–$25,771 | 0 | |
| $24,170 | 1.2% | $4,028 | $1,648 | $1,068–$15,081 | 0 | |
| $10,721 | 0.5% | $1,787 | $0 | $0–$10,382 | 4 | |
|
$193,917 | 9.3% | $32,320 | $22,869 | $6,140–$74,325 | 0 |
| Total | $2,081,930 | 100% | $346,988 | $213,314 | $104,665–$893,877 |
References
Unpublished data provided by the Department↩︎




